- Etiology: progressive leukoencephalopathy, autosomal recessive, lysosomal storage disorder due to arylsulfatase-A deficiency with resultant accumulation of sulfatides which are membrane lipids, the accumulation of sulfatides in oligodendroglia and Schwann cells may lead to their ultimate death and myelin instability, abnormal accumulation of sulfatide in the gall bladder leads to a proliferative response in the gallbladder epithelium
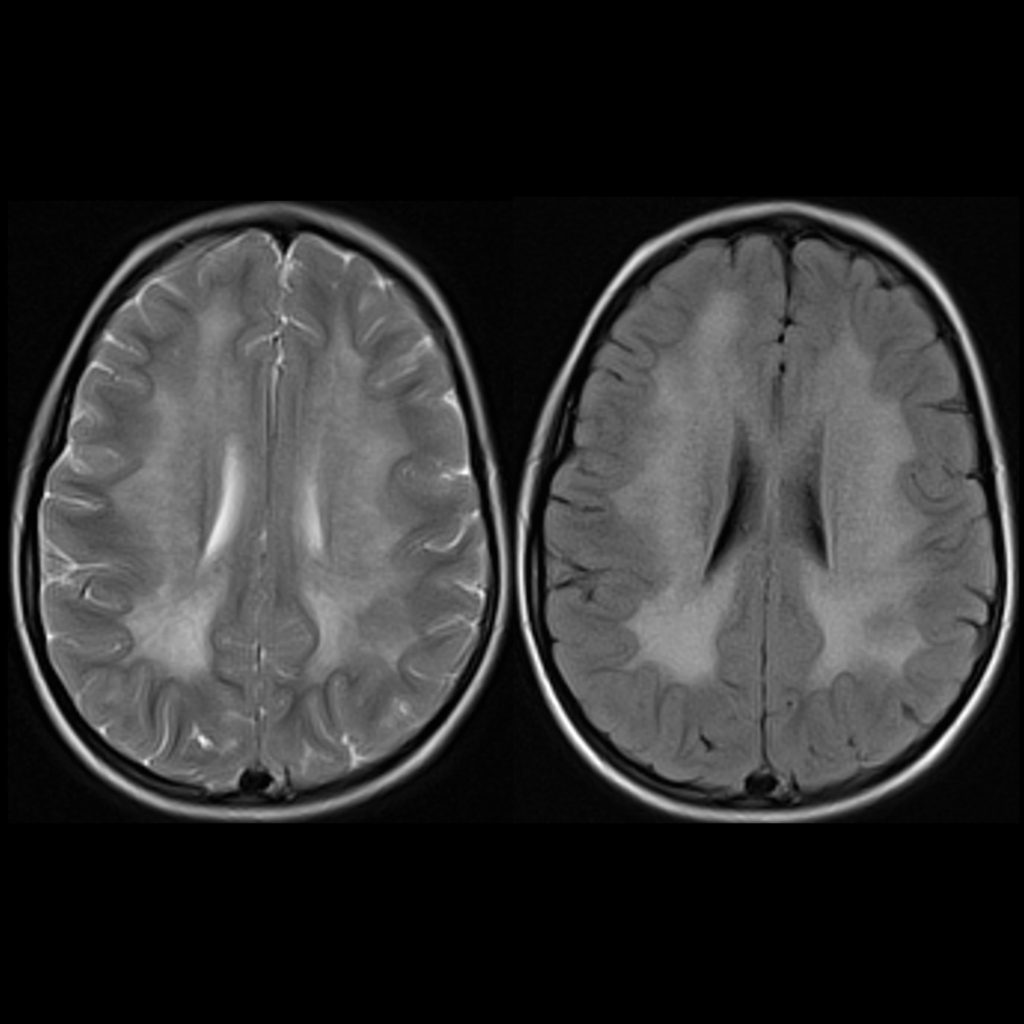
- MRI: bilateral symmetric and confluent periventricular white matter T1 hypointensity and T2 hyperintensity = butterfly pattern, starts at core of centrum semiovale sparing periventricular white matter and subcortical U-fibers, tigroid or leopard patterns due to relative sparing of perivenular myelin
- DDX:
- Complications:
- Treatment:
- Clinical: most common leukodystrophy, late infantile (most common) / juvenile / adult forms, 40% present with infantile subtype at 6 months old – 3 years old with unsteady gait due to muscle hypotonia and 40% present with juvenile subtype at 4-16 years old
Radiology Cases of Metachromatic Leukodystrophy